
Page 204 - Personnel Policy and Procedures Manual
P. 204
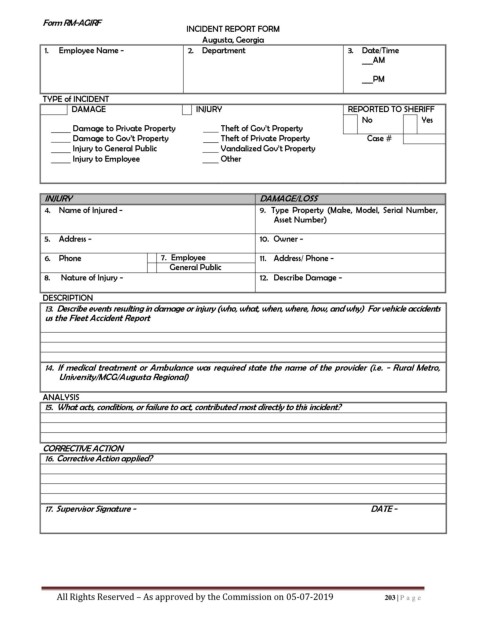
Form RM-AGIRF
INCIDENT REPORT FORM
Augusta, Georgia
1. Employee Name - 2. Department 3. Date/Time
___AM
___PM
TYPE of INCIDENT
DAMAGE INJURY REPORTED TO SHERIFF
No Yes
Damage to Private Property Theft of Gov’t Property
Damage to Gov’t Property Theft of Private Property Case #
Injury to General Public Vandalized Gov’t Property
Injury to Employee Other
INJURY DAMAGE/LOSS
4. Name of Injured - 9. Type Property (Make, Model, Serial Number,
Asset Number)
5. Address - 10. Owner -
6. Phone 7. Employee 11. Address/ Phone -
General Public
8. Nature of Injury - 12. Describe Damage -
DESCRIPTION
13. Describe events resulting in damage or injury (who, what, when, where, how, and why) For vehicle accidents
us the Fleet Accident Report
14. If medical treatment or Ambulance was required state the name of the provider (i.e. - Rural Metro,
University/MCG/Augusta Regional)
ANALYSIS
15. What acts, conditions, or failure to act, contributed most directly to this incident?
CORRECTIVE ACTION
16. Corrective Action applied?
17. Supervisor Signature - DATE -
All Rights Reserved – As approved by the Commission on 05-07-2019 203 | P a g e